Overview of double-hit lymphoma (& triple-hit lymphoma)
Double-hit lymphoma (DHL) and triple-hit lymphoma (THL) or also known as ‘high grade B-cell lymphoma’ are aggressive (fast-growing) lymphomas with signs and symptoms that may be similar to those ofdiffuse large B-cell lymphoma. Other features include both diffuse large B-cell lymphoma and Burkitt lymphoma and are unclassifiable into a specific type of high-grade B-cell lymphoma.
Double-hit lymphoma (DHL) occurs in around 5-10% of all people who are diagnosed with diffuse large B-cell lymphoma (DLBCL). Triple-hit lymphoma (THL) accounts for around 2% of all diffuse large B-cell lymphomas.
Double-hit lymphoma (DHL) is a subtype of B-cell NHL formally called “High Grade B-cell lymphoma with rearrangements of MYC and BCL2 and/or BCL6”. It is characterised by rearrangements (parts of genes switch places within chromosomes) in two particular genes. One rearrangement involves the MYC gene, and the other involves the BCL2 gene or, less commonly, the BCL6 gene.
Triple-hit lymphoma (THL): is a rarer subtype of B-cell NHL, where rearrangements are present in all three genes (MYC, BCL2 and BCL6) and the condition is called ‘triple-hit lymphoma’.
These changes are usually detected only if the pathologist is asked to check, using a specialist test called FISH (fluorescence in-situ hybridisations) to confirm a diagnosis of double-hit lymphoma.
The normal role of these important genes in cell regulation includes:
- MYC gene regulates approximately 15% of human genes and has a role in the progression of the cell cycle, apoptosis (programmed cell death) and cellular result in rapid growth of lymphoma cells
- BCL2 gene regulates cell death (apoptosis) by either inducing it or inhibiting it. In DHL, the changes in this gene result in an anti-apoptotic effect in lymphoma cells, leading to their prolonged survival.
- BCL6 gene has a role in regulating activation, survival, DNA damage response and cell cycle arrest.
They do however act differently in certain ways and more resistant, therefore they have been categorized as their own subtype. Double-hit lymphoma and triple-hit lymphoma often start in extranodal sites (outside the lymph nodes). They seem to behave more aggressively than the more common diffuse large B-cell lymphoma (DLBCL) and may need more intensive treatment.
What is double-expressor lymphoma?
Double expresser lymphoma (DEL) is an aggressive (fast-growing) B-cell non-Hodgkin lymphoma (NHL). Double expresser lymphoma (DEL) is different from double-hit lymphoma (DHL) and is a subtype of diffuse large B-cell lymphoma (DLBCL). Double-expressor lymphoma (DEL) has increased expression of MYC and BCL2 proteins not related to underlying chromosomal rearrangements.
This does not imply that a patient has double-hit lymphoma (DHL) and these double expresser lymphomas (DEL) generally are thought to have a better prognosis, although worse to standard diffuse large B-cell lymphoma.
There is not a standard treatment for DEL either and often doctors will treat with more intense immunochemotherapy as they do DHL.
Treatment and prognosis
There is a poorer prognosis when treated with standard chemoimmunotherapy, that is used in the treatment of diffuse large B-cell lymphoma, and so can be treated with more intense treatments. Because double-hit and triple-hit lymphoma are fairly new classifications of lymphoma, ongoing research is helping doctors learn more about the best ways to treat this disease.
Who is affected by double-hit lymphoma (DHL) & triple-hit lymphoma (THL)?
Double-hit lymphoma (DHL) occurs in around 5-10% of all people who are diagnosed with diffuse large B-cell lymphoma (DLBCL). Triple-hit lymphoma (THL) accounts for around 2% of all diffuse large B-cell lymphomas. DHL/THL often develop in older people, aged over 60 years.
Double-hit lymphoma (DHL) and triple-hit lymphoma (THL) may occur in people with a history of indolent (slower growing) lymphoma, called follicular lymphoma. This is known as transformed lymphoma (changes to a fast-growing lymphoma over time).
Symptoms of double-hit (DHL)
Double-hit lymphoma (DHL) or triple-hit lymphoma (THL) can start anywhere in the body and can have many different symptoms. They often start in extranodal sites (outside of the lymph nodes). The exact symptoms they cause depend on the type of lymphoma and where it is located in the body.
About half of all people with double-hit or triple-hit lymphoma have lymphoma in the bone marrow. Around 10% have symptoms caused by lymphoma in their central nervous system (brain and spinal cord). Most people have advanced stage disease at diagnosis.
Most symptoms of lymphoma can also be symptoms of many other illnesses. Because the symptoms can be very general, it can be hard to diagnose. Most common symptoms include:
- Painless lumps in the neck, groin or armpit, that are enlarged lymph nodes.
- Fatigue (tiredness or lack of energy)
- Loss of appetite
- Itchy skin
B symptoms are what doctors call the following symptoms and can include:
- Night sweats (drenching sleepwear & bedding)
- Persistent fevers (especially at night (>38C)
- Unexplained weight loss
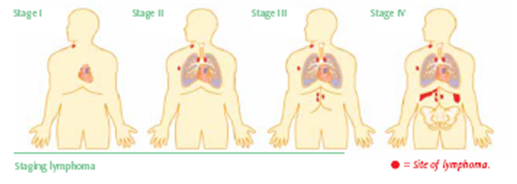
Diagnosis and Staging
A biopsy is always required for diagnosis of lymphoma. A biopsy is a surgical procedure to remove part of or all of an affected lymph node or other tissue to look under the microscope by a pathologist to see what the cells look like. The biopsy can be done under local or a general anaesthetic depending on what part of the body is being biopsied. The biopsy can be one of three ways:
- Fine needle aspirate
- Core needle biopsy
- Excisional node biopsy
An excisional node biopsy is the best investigative option, as it collects the most adequate amount of tissue to be able to do the necessary testing for a diagnosis.
Waiting for results can be a difficult time. It may help to talk to family, friends or a specialist nurse.