








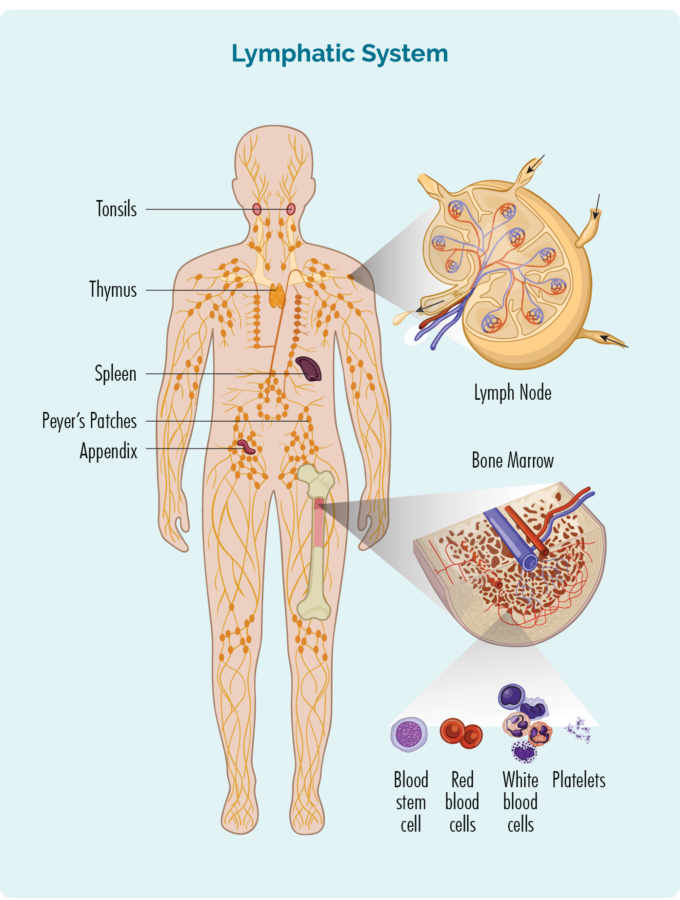
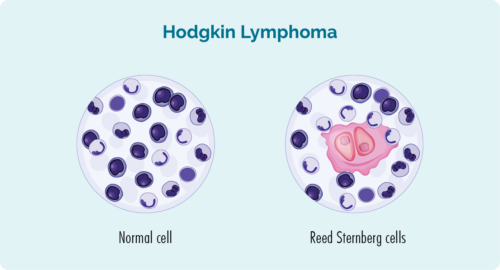
What does a Reed-Sternberg cell look like?
Here’s a picture to show you normal cells look like, and what Reed-Sternberg lymphoma cells look like.
Hodgkin lymphoma usually grows quickly, so it is sometimes called aggressive. But the good thing about aggressive Hodgkin lymphoma is that it often responds well to treatment, because the treatment is designed to attack the fast-growing cells.
For this reason, there is a very good chance you will be cured after treatment. That means you will no longer have cancer.

The first symptom you might get if you have HL can be a lump, or several lumps that keep growing. These lumps can be on your neck, armpit, groin or abdomen (your tummy area). Lymph nodes in your abdomen may be harder to see and feel, because they are much deeper in your body than other lymph nodes.
The lumps are caused by your lymph nodes filling up with lymphoma cells, which makes them swell up. It usually is not painful but sometimes, if the swollen lymph nodes are putting pressure on other parts of your body it may cause some pain.
Where else can Hodgkin Lymphoma be found?
Sometimes, Hodgkin lymphoma can spread to other parts of your body such as your:
- lungs – your lungs help you breathe
- liver – your liver helps you to digest food, and cleans your body so you don’t build up harmful toxins (poisons) in your body
- bones
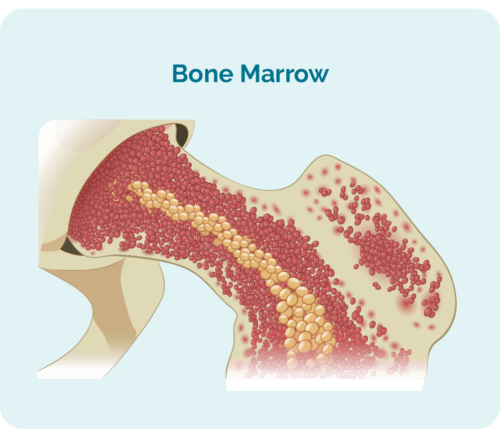
- bone marrow (this is in the middle of your bones and is where your blood cells are made).
- other organs that help your body work properly.
If your lymphoma cells spread to other areas of your body, it can be called advanced stage. We will talk about stages of HL more a little later.


There are many different types of lymphoma. They are usually grouped into Hodgkin lymphoma or non-Hodgkin lymphoma. Hodgkin lymphoma is then grouped into:
- Classical Hodgkin Lymphoma (cHL) or
- Nodular Lymphocyte Predominant Hodgkin Lymphoma (NLPHL)
Most of you will have cHL, with only 1 out of every 10 children and teenagers with HL having the NLPHL subtype.
How does my Doctor know what subtype I have?
It is important for your doctor to work out which one you have, because the types of treatment and medicines you get may be different to someone with a different subtype to you.
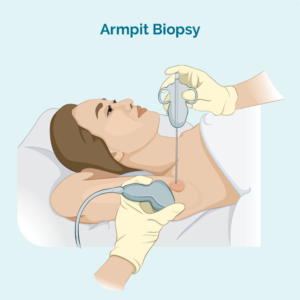
To find out what type of HL you have, your doctor will want to do some different tests. They will want to take samples of your swollen lymph nodes to test them and see what type of cells are in there. When the doctor takes a sample, it is called a biopsy. Depending on how old you are, and where your swollen lymph nodes are your, you might have your biopsy in the doctor’s room, in an operating room at the hospital or in a radiology department. Your doctor will you know where you and your parents/guardians need to go.
Biopsy
A biopsy can be done as an operation at the hospital. Your doctors and nurses will be very careful and make sure you are as comfortable as possible while they do the biopsy. You might even get some medicine that helps you to sleep during the biopsy, or make the spot they do the biopsy feel numb. This medicine is called an anaesthetic.
Once you have the biopsy, the sample will be taken to a laboratory where scientists will use different types of equipment like microscopes and special lights to look at the cells in the biopsy. By using these different types of equipment, they can see different parts of the lymphoma cells and help your doctor to diagnose what subtype of HL you have.
Some types of biopsies you might have include:
Core or fine needle biopsy
The doctor or nurse practitioner will put a needle into your swollen lymph node and remove a small sample of of the lymph node. You will have some medicine to numb the area so it doesn’t hurt, and depending on your age, you may even some medicine to make you sleepy so you can stay really still.
If the lymph node is deep inside your body and they can’t feel it, the doctor may use a ultrasound or specialised x-ray (imaging) guidance to help them see when they take the biopsy.
Excisional node biopsy
this may involve a more invasive day surgery to remove lymph nodes in other areas of your body that can’t be reached by a needle. This is usually done under general anaesthetic and you will have a small wound and stitches.
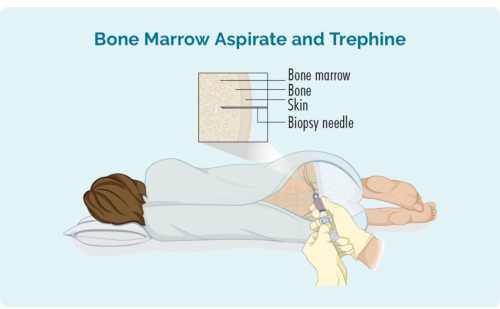
Bone marrow biopsy
A bone marrow biopsy involves the doctor placing a needle into your lower back and into your hip bone where your blood cells are made. There are two samples the doctor will take from this space including:
- Bone marrow aspirate (BMA): this test takes a small amount of the liquid found in the bone marrow space
- Bone marrow aspirate trephine (BMAT): this test takes a small sample of the bone marrow tissue
It can take a couple of weeks to get your results back. Waiting for results can be a stressful time for you and your loved ones. It is important for you and your mob or family and friends to reach out and talk to someone you trust during this time. If you’re not sure who to talk to, or if you have questions, you can always call or email our lymphoma care nurses.
For details on how to contact them please click on the blue contact us button at the bottom of the screen.

NS-cHL is more common in older children and teenagers. Almost half of everyone with classical Hodgkin lymphoma will have this NS-cHL subtype.
Boys and girls can both get NS-cHL, but it is a little bit more common in girls.
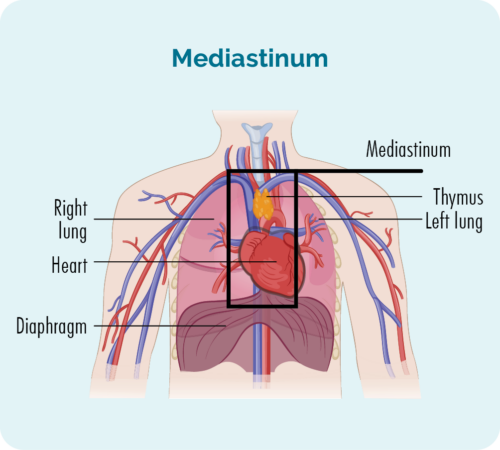
NS-cHL usually starts in lymph nodes deep inside your chest in an area called your mediastinum. You may or may not be able feel you swollen lymph nodes, but some other symptoms you may get with type of HL include:
- coughing
- pain or an uncomfortable feeling in your chest
- feeling short of breath
NS-cHL can also start, or spread to other parts of your body such as your spleen, lungs, liver, bone or bone marrow.
Mixed cellularity classical Hodgkin Lymphoma (MC-cHL) is more common in children less than 10 years of age. But it can still affect children and teenagers of any age. If you have MC-cHL, you may notice new lumps just under your skin. This is because the lymphoma cells gather and grow in your lymph nodes in the fatty tissue just under your skin. We all have this fatty tissue and it helps to protect our organs underneath, and keep us warm during cold weather. Some lymphoma cells might also be found in your other organs.
MC-cHL can sometimes be tricky for your doctor to diagnose because it looks like a different subtype of lymphoma called peripheral T-cell lymphoma. For this reason, your doctor may want to do extra tests to make sure you have MC-cHL so they can give you the right medicines.
Lymphocyte-rich classical Hodgkin lymphoma (LR-cHL) is a rare subtype of HL, so not many of you will have this subtype. But for those of your that do, it usually responds very well to your treatment. Most of you will be cured after your treatment. Most of you will notice some lumps just under your skin if you have LR-cHL because the lymphoma cells grow in the lymph nodes just under your skin.
LR-cHL can also be tricky for your doctor to diagnose because it sometimes look like a different type of HL called Nodular lymphocyte predominant Hodgkin Lymphoma (NLPHL). Both LR-cHL and NLPHL look the same, but different medicines are used to get rid of them.
Lymphocyte-depleted classical Hodgkin Lymphoma (LD0cHL) is probably the least common subtype of classical Hodgkin lymphoma in children and teenagers. It is more common if you have an infection called human immunodeficiency virus (HIV) or if you have ever had an infection called Epstein-Barr virus (EBV).
You may not have unusual lumps or swollen lymph nodes if you have LD-cHL because it often grown in the middle of your bones in a place called your bone marrow. This is the place where your blood cells are made. However, it can also start deep in your abdomen (or tummy) area, so the lumps may be too deep for you to feel.
Nodular Lymphocyte Predominant Hodgkin Lymphoma (NLPHL)
Nodular Lymphocyte Predominant Hodgkin Lymphoma (NLPHL) is a very rare subtype of HL, but it is more common in children younger than 10 years of age.
Your doctor can diagnose your with NLPHL if your cells look a certain way. It may seem funny, but we sometimes say the lymphoma cells in NLPHL look like popcorn. Take a look at the picture and you’ll see what we mean.

How is Nodular Lymphocyte Predominant Hodgkin Lymphoma (NLPHL) different to classical Hodgkin Lymphoma?
NLPHL grows more slowly than Classical Hodgkin Lymphoma. If you have NLPHL , you may be cured after treatment which means the lymphoma will go away and never come back. But, for some of you, it may come back. Sometimes it can come back quickly, and other times you might live without lymphoma for many years.
If your NLPHL comes back it is called a relapse. The only sign of a relapse might be a swollen lymph node that does not go away. This might be in your neck, armpit, groin or other area of your body. If you get other symptoms, they will be similar to the symptoms we listed above.
Staging looks at where the HL is. Remember earlier we talked about your lymphocytes. We found out that although they are made in your bone marrow and live in your lymphatic system, they can also travel to any part of your body. Because the cells of your lymphoma are cancerous lymphocytes, the HL can also be in your bone marrow, lymphatic system or any other part of your body.
Staging Tests and Scans
So, your doctor will order some scans to take pictures of the inside of your body to see where these HL cells are hiding. These scans might include:
CT scan (this stands for computed tomography scan)
This is like a special X-ray that gives a detailed picture of everything inside your chest, abdomen (tummy area) and pelvis (near your hip bones). Your doctor will be able to see any swollen lymph nodes or tumours in these areas on this scan.
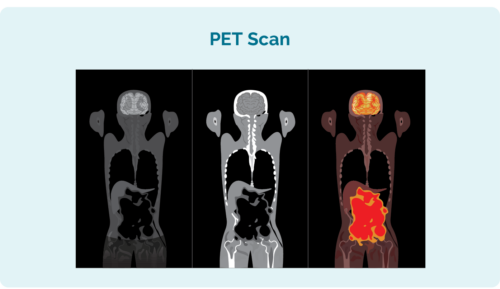
PET scan (this stands for Positron Emission Tomography scan)
This scan looks inside your whole body. The areas that have lymphoma look brighter than other area. You will need to have needle in your hand or arm for this one because they will inject some fluid that helps the lymphoma cells light up on the computer image. The nurses are very good at doing this and will take special care to make sure it doesn’t hurt too much.
MRI scan (This stands for Magnetic Resonance Imaging)
This scan uses magnets inside a machine to take pictures of the inside of your body. It doesn’t hurt, but because there are magnets swirling around in the machine it can be very noisy. Some people don’t like these noises so you might have some medicine to make you a little sleepy during the scan, so it doesn’t worry you.
How is my HL stage numbered?
Staging is numbered from the number one to the number four. If you have stage one or two you will have an early-stage HL. If you have stage three or four, you will have an advanced stage HL.
Advanced stage HL can sound scary. But, because your lymphocytes travel all around your body, lymphoma is considered a “systemic” disease. So, advanced lymphomas including HL are very different to other cancers with advanced disease. Many solid tumours, such as tumours in the brain, breast, kidneys and other places cannot be cured if they are advanced.
But many advanced stage lymphomas can be cured with the right treatment, and this is often the case for children and teenagers with HL.
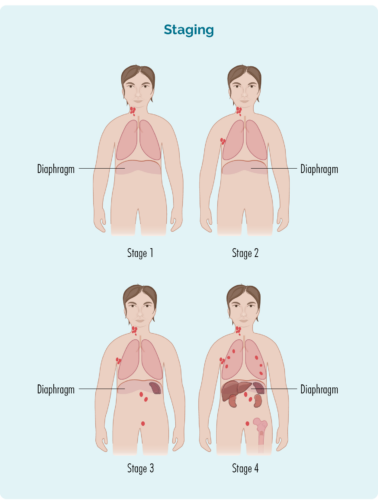
This picture is a good example of how the different stages might look. The red parts show where the lymphoma might be in each stage – yours may be a little different, but will follow roughly the same pattern.
stage 1 | Your HL is in one lymph node area, either above or below your diaphragm* |
stage 2 | Your HL is in two or more lymph node areas, but on the same side of your diaphragm* |
stage 3 | Your HL is in at least one lymph node area above and at least one lymph node area below your diaphragm* |
stage 4 | Your HL is in multiple lymph nodes areas, and has spread to other parts of your body, such as your bones, lungs, or liver |
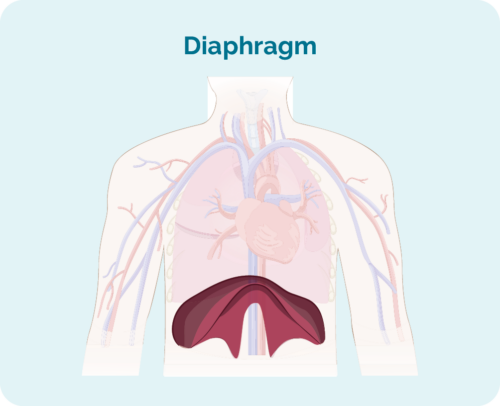
What is your diaphragm?
Your diaphragm is a dome shaped muscle that separates the organs in your chest, form the organs in your abdoment. It also helps you to breathe by helping your lungs move up and down.
Other important things to know about your stage
As well as a staging number, you might be given a letter after the number.
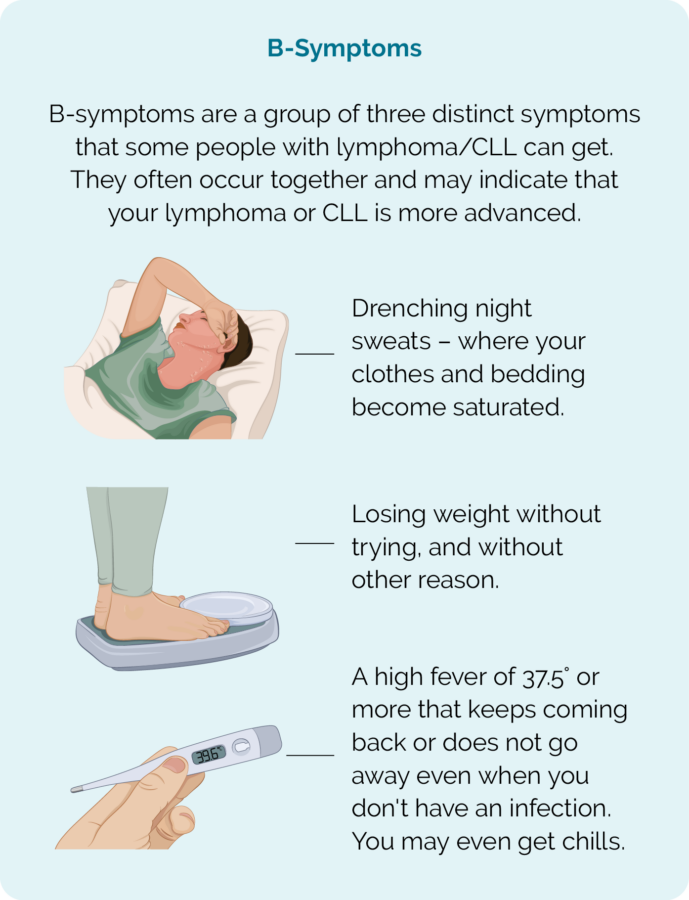
Do you remember what we said earlier about the B-symptoms? They are a group of symptoms that can happen together when you have lymphoma. They include:
- Drenching night sweats that wet your clothes and bedding
- Fevers and chills
- Losing weight without trying
If you have these B-symptoms you will have a “B” after your staging number, but if you don’t have B-symptoms you will have an “A” after your staging number.
If one of your organs, such as your lungs, liver or bones have HL you will have the letter “E” after your staging number.
If you have a lymph node or tumour that is more than 10cm in size it is considered a bulky disease. If you have bulky disease, you will have the letter “X” after your staging number
Finally, if your spleen has HL in it, you will have the letter “S” after your staging number. Your spleen helps to keep your blood clean, and is a major organ of your immune system. It is where a lot of your white blood cells live and where your B-cell lymphocytes make a lot of antibodies to fight germs.
See what these different things can mean in the table below.
Meaning | Importance |
|
|
|
|
|
|
Grading helps your doctor make good choices about the treatments they offer you.
Just like staging, your grade will be given as a number from one to four. It might be written as G1, G2, G3 or G4. When your lymphocytes become cancerous, they begin to look different to your normal lymphocytes. If you have a low grade lymphoma such as G1, the cells might be growing slowly and only be a little different to your normal lymphocytes, but with a higher grade, they grow very fast and can look nothing like your normal cells. The more different they look, the less they are able to work properly.
As we mentioned earlier, you will have biopsies of your swollen lymph nodes or tumour. As well as the biopsies mentioned above, you will have blood tests and you may also have another type of biopsy called a bone marrow biopsy.
Bone marrow biopsies are where the doctor puts a needle into your back and into your hip bone to take out some of the bone marrow to send to pathology for testing. This might sound awful, but you will be given a local anaesthetic to the area to make it numb, and you might even be given medicine to make you sleepy so you don’t feel or remember having the bone marrow biopsy done.
Here is on overview of each grade:
- G1 – low grade – your cells look close to normal and they grow and spread slowly.
- G2 – intermediate grade – your cells are starting to look different but some normal cells exist and they grow and spread at a moderate rate.
- G3 – high grade – your child’s/ your cells look fairly different with a few normal cells and they grow and spread faster.
- G4 – high grade – your child’s/ your cells look most different to normal and they grow and spread the fastest
Starting Treatment for Hodgkin Lymphoma (HL)
When you first start treatment, you might feel a bit like the man in this photo. But knowing what to expect can make it a little easier. So keep reading and let us tell you about what might happen.
The first time you have a type of treatment it is called first-line treatment. When you start treatment, you will have it in cycles. That means you will have the treatment, then a break, then another round (cycle) of treatment.
It’ss usually given as an infusion into your vein. Most children and teenagers will need to have a device called a tunnelled catheter that the medicine is put through. The tunnelled catheter is used so you won’t need to have a needle every time you have treatment or a blood test. You can find information on tunnelled catheters by clicking on the button below.

