


To understand DLBCL you need to know a bit about your B-Cell lymphocytes.
B-Cell lymphocytes:
- Are a type of white blood cell
- Fight infection and diseases to keep you healthy.
- Remember infections you had in the past, so if you get the same infection again, your body’s immune system can fight it more effectively and quickly.
- Are made in your bone marrow (the spongy part in the middle of your bones), but usually live in your spleen and your lymph nodes. Some live in your thymus and blood too.
- Can travel through your lymphatic system, to any part of your body to fight infection or disease.

DLBCL develops when some of your B-cells become cancerous. They grow uncontrollably, are abnormal, and do not die when they should.
When you have DLBCL your cancerous B-cell lymphocytes:
- Will not work as effectively to fight infections and disease.
- Can become larger than they should and can look different to your healthy B-cells.
- Can cause lymphoma to develop and grow in any part of your body.
- Are spread out (diffuse) rather than grouped closely together.
Although DLBCL is usually a fast growing (aggressive) lymphoma, many people with DLBCL can be cured with treatment, even if you are diagnosed with an advanced stage. An advanced stage of lymphoma is very different to advanced stages of other cancers which cannot be cured.


Staging refers to how much of your body is affected by your lymphoma – or how far it has spread from where it first started.
B-cells can travel to any part of your body. This means that lymphoma cells (the cancerous B-cells), can also travel to any part of your body. You will need to have more tests done to find this information. These tests are called staging tests and when you get results, you will find out if you have stage one (I), stage two (II), stage three (III) or stage four (IV) DLBCL.
Your stage of DLBCL will depend on:
- How many areas of your body have lymphoma
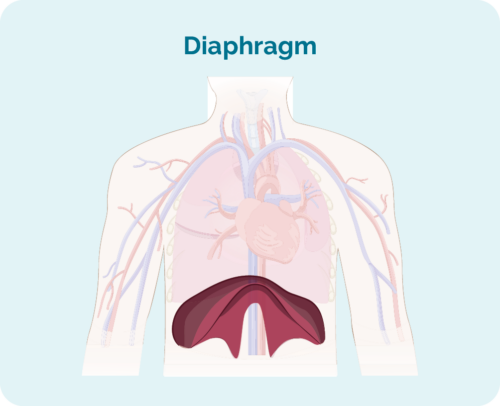
- Where the lymphoma is including if it is above, below or on both sides of your diaphragm (a large, dome-shaped muscle under your rib cage that separates your chest from your abdomen)
- Whether the lymphoma has spread to your bone marrow or other organs such as your liver, lungs, skin or bone.
Stages I and II are called ‘early or limited stage’ (involving a limited area of your body).
Stages III and IV are called ‘advanced stage’ (more widespread).
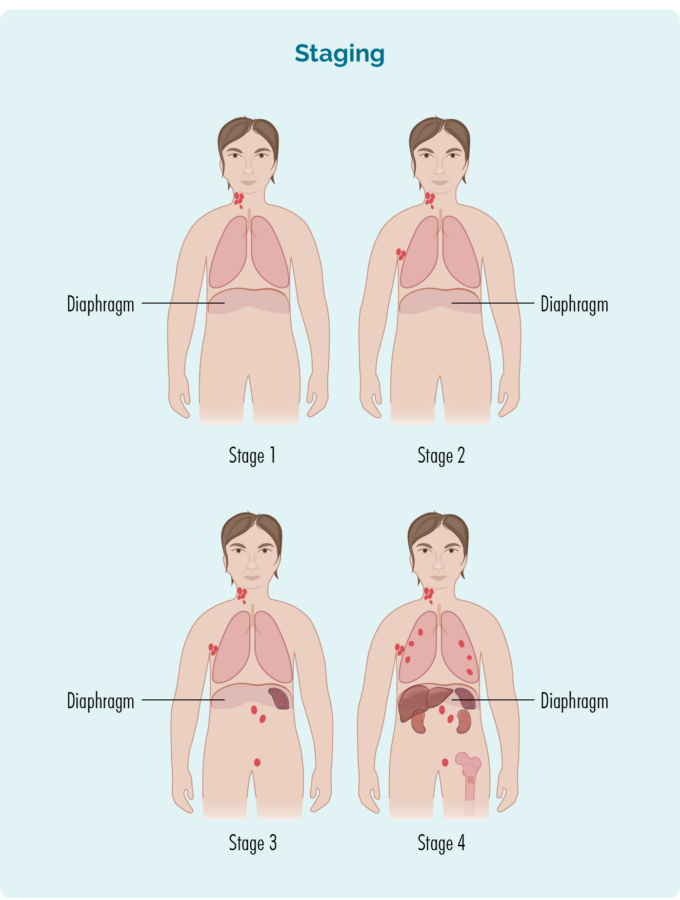
Stage 1 | One lymph node area is affected, either above or below the diaphragm*. |
Stage 2 | Two or more lymph node areas are affected on the same side of the diaphragm*. |
Stage 3 | At least one lymph node area above and at least one lymph node area below the diaphragm* are affected. |
Stage 4 | Lymphoma is in multiple lymph nodes and has spread to other parts of the body (e.g. bones, lungs, liver). |
Extra staging information
Your doctor may also talk about your stage using a letter, such as A,B, E, X or S. These letters give more information about the symptoms you have or how your body is being affected by the lymphoma. All this information helps your doctor find the best treatment plan for you.
Letter | Meaning | Importance |
A or B |
|
|
E & X |
|
|
S |
|
(Your spleen is an organ in your lymphatic system that filters and cleans your blood, and is a place your B-cells rest and make antibodies) |
Tests for staging
To find out what stage you have, you may be asked to have some of the following staging tests:
Computed tomography (CT) scan
These scans takes pictures of the inside of your chest, abdomen or pelvis. They provide detailed pictures that provide more information than a standard X-ray.
Positron emission tomography (PET) scan
This is a scan that takes pictures of the inside of your whole body. You will be given and needle with some medicine that cancerous cells – such as lymphoma cells absorb. The medicine that helps the PET scan identify where the lymphoma is and the size and shape by highlighting areas with lymphoma cells. These areas are sometimes called “hot”.
Lumbar puncture
A lumbar puncture is a procedure done to check if you have any lymphoma in your central nervous system (CNS), which includes your brain, spinal cord and an area around your eyes. You will need to stay very still during the procedure, so babies and children may have a general anaesthetic to put them to sleep for a little while when the procedure is done. Most adults will only need a local anaesthetic for the procedure to numb the area.
Your doctor will put a needle into your back, and take out a little bit of fluid called “cerebral spinal fluid” (CSF) from around your spinal cord. CSF is a fluid that acts a bit like a shock absorber to your CNS. It also carries different proteins and infection fighting immune cells such as lymphocytes to protect your brain and spinal cord. CSF can also help drain any extra fluid you may have in your brain or around your spinal cord to prevent swelling in those areas.
The CSF sample will then be sent to pathology and checked for any signs of lymphoma.
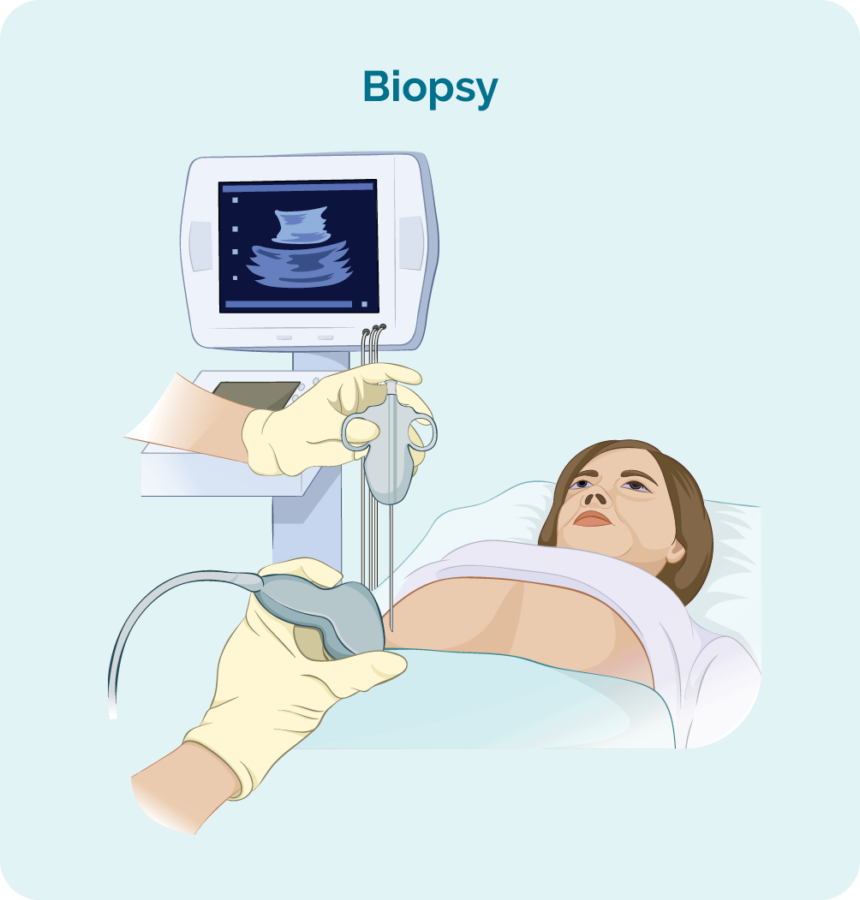
Bone marrow biopsy
- Bone marrow aspirate (BMA): this test takes a small amount of the liquid found in the bone marrow space.
- Bone marrow aspirate trephine (BMAT): this test takes a small sample of the bone marrow tissue.

The samples are then sent to pathology where they are checked for signs of lymphoma.
The process for bone marrow biopsies can differ depending on where you are having your treatment, but will usually include a local anaesthetic to numb the area.
In some hospitals, you may be given light sedation which helps you to relax and can stop you from remembering the procedure. However many people do not need this and may instead have a “green whistle” to suck on. This green whistle has a pain killing medication in it (called Penthrox or methoxyflurane), that you use as needed throughout the procedure.
Make sure you ask your doctor what is available to make you more comfortable during the procedure, and talk to them about what you think will be the best option for you.
More information on bone marrow biopsies can be found at our webpage here.
Your lymphoma cells have a different growth pattern, and look different to normal cells. The grade of your lymphoma is how quickly your lymphoma cells are growing, which affects the way look under a microscope. The grades are Grades 1-4 (low, intermediate, high). If you have a higher grade lymphoma, your lymphoma cells will look the most different from normal cells, because they are growing too quickly to develop properly. An overview of the grades is below.
- G1 – low grade – your cells look close to normal, and they grow and spread slowly.
- G2 – intermediate grade – your cells are starting to look different but some normal cells exist, and they grow and spread at a moderate rate.
- G3 – high grade – your cells look fairly different with a few normal cells, and they grow and spread faster.
- G4 – high grade – your cells look most different to normal, and they grow and spread the fastest.
All this information adds to the whole picture your doctor builds to help decide the best type of the treatment for you.
It is important that you talk to your doctor about your own risk factors so you can have clear idea of what to expect from your treatments.
Primary mediastinal B-cell lymphoma (PMBCL) is a rare aggressive (fast-growing) type of non-Hodgkin Lymphoma. It used to be classified as a sub-type of DLBCL, but has now been reclassified by the World Health Organisation as a subtype on its own.
For more information on PMBCL, please see our Primary Mediastinal B – cell lymphoma (PMBCL) webpage here, or our factsheet here.
T-cell/histiocyte rich B-cell lymphoma (T/HRBCL) is a rare subtype of DLBCL that can be very difficult for your doctor to diagnose. It is difficult to diagnose because it looks a lot like two other subtypes of lymphoma. For this reason, some people with T/HRBCL can get a wrong diagnosis of Hodgkin’s lymphoma or peripheral T-cell lymphoma, before getting the right diagnosis. You will need some special tests to diagnose T/HRBCL called immunohistochemistry tests. This is a special test done on your biopsies so your doctor can learn more about your lymphoma.
T-cells are another type of lymphocyte cell that helps your immune system remember infections you’ve had in the past. They help to keep your immune system in check so it doesn’t work too hard, and also supports other cells of your immune system to work more effectively. Histiocytes are also a type or immune cell called a phagocyte. Phagocytes help to protect you from infection and disease because they recognise the bad cells and eat them.
If you have T/HRBCL – you have too many T-cells and histiocytes (which is why it’s called “rich” – T/HR) while also having cancerous B-cell lymphocytes (BCL).
Standard treatment for T/HRBCL is the same as most other subtypes of diffuse large B-cell lymphoma (DLBCL), discussed later on this webpage.
EBV-positive DLBCL not otherwise specified is a subtype of DLBCL that can occur in young people, but most commonly affects people over 50 years of age. It occurs in some people who have had a virus called Epstein-Barr virus (EBV), which affects B-cells. EBV causes glandular fever (also called “mono” or the kissing disease). However, only a very small number of people who have had EBV go on to develop EBV-positive DLBCL. Unfortunately we currently have no way of knowing who will develop this lymphoma after infection with EBV.
Symptoms will depend on where your lymphoma is growing. It usually starts in your lymph nodes (called nodal lymphoma) which can cause a new lump to come up. This is usually in your neck, armpit, groin or tummy, but can be anywhere in your body.
Other places it can grow and the symptoms associated with it are similar to those listed above in table one.
Standard treatment for intravascular large B-cell lymphoma is the same as most other subtypes of diffuse large B-cell lymphoma (DLBCL), discussed later on this webpage.
ALK-positive large B-cell lymphoma is a very rare subtype of DLBCL. It can affect people of any age and is more common in men. The lymphoma cells have a gene mutation that makes a protein on the surface of their B-Lymphocyte cells called ‘anaplastic large-cell kinase’ (ALK).
Most subtypes of DLBCL have a protein on the lymphoma cells called CD20. However, ALK positive large B-cell lymphomas do not usually have the CD20 protein. For this reason, treatment will be slightly different from other DLBCL subtypes. Although most of the medications will be the same, if you have this subtype, you will not receive a monoclonal antibody medicine called rituximab. Rituximab only works when CD20 is found on the lymphoma cells. So, if you’re wondering why you may not be getting the extra medicines other patients are getting….this may be the reason.
ALK-positive large B-cell lymphoma usually starts in your lymph nodes, so a common symptom you might experience is swollen lymph nodes.
However, it can also start in areas outside of your lymphatic system, including your:
- tongue
- nasopharynx (the area at the back of your nose and mouth)
- ovaries
- liver
- breasts
- bones
- stomach
- brain or epidural space (an area surrounding your spine)
Your symptoms will related to where the lymphoma is growing.
Intravascular large B-cell lymphoma is a rare form of an *extra-nodal DLBCL. It mostly affects older adults between 50-70 years of age. This subtype occurs equally in both men and women. The lymphoma cells are found within the inside lining of your small blood vessels. These small blood vessels are called capillaries.
Intravascular large B-cell lymphoma does not usually cause enlarged lymph nodes. It may affect small blood vessels in your skin or your brain. You may have central nervous system (CNS) symptoms. Your central nervous system includes your brain and spinal cord, so the symptoms you experience may include:
- confusion
- seizures
- dizziness
- weakness
Other symptoms you may experience specific to your subtype include:
- reddened patches or lumps on your skin
- an enlarged liver and/or spleen
These symptoms are in addition to the general lymphoma symptoms listed above.
Standard treatment for intravascular large B-cell lymphoma is the same as most other subtypes of diffuse large B-cell lymphoma (DLBCL), discussed later on this webpage.
*Extra-nodal means your lymphoma developed outside of your lymph nodes.
Primary Central Nervous System Lymphoma (PCNSL) is a rare subtype of DLBCL that is considered aggressive because it grows quickly. It is more common in people aged between 50 and 60 years of age, but can occur at any age.
If you have PCNSL your lymphoma likely started in your central nervous system, which includes your brain and spinal cord.
In more than 9 out 10 people that have PCNSL the lymphoma develops in the brain, spinal cord, eye or leptomeninges (the inner two membranes surrounding the brain and spinal cord).
The most common site is in the brain.
If your lymphoma has started in other parts of your body first then at some stage has spread to the brain or spinal cord, it is referred to as ‘secondary’ CNS lymphoma (SCNSL).
Treatment and management of PCNSL is different from other subtypes of DLBCL as the standard treatments cannot reach your brain and spinal cord. You can read more about the treatments for PCNSL later in the webpage under the heading Treatments.

Cutaneous (skin) B-cell lymphoma is a rare subtype of DLBCL that develops from the B-cells in your skin. Less than 1 out of 100 people with NHL will be diagnosed with this subtype.
For you doctor to diagnose you with this subtype, the lymphoma needs to be only affecting your skin.
Because this lymphoma starts in your skin, the main symptoms you may notice include are lumps, patches or a rash anywhere on your skin.
As cutaneous B-cell lymphomas are managed differently to other DLBCL subtypes, we have dedicated a different webpage to these subtypes.
You can find more specific information about cutaneous B-cell lymphoma here.
Please note that if you have been diagnosed with another subtype of DLBCL and it has spread to your skin, you should continue to look at the information on that first subtype. If the lymphoma has spread to your skin after starting somewhere else, it is considered secondary cutaneous lymphoma. Primary and secondary cutaneous lymphomas are managed differently.
Additionally, if you have cutaneous T-cell lymphoma, this is different again.
You can find more information on cutaneous T-cell lymphoma here.

Supportive care is given to patients and families facing serious illness. Supportive care can help patients have fewer symptoms, and actually get better faster by paying attention to those aspects of their care.
For some of you with DLBCL, your leukemic cells may grow uncontrollably and crowd your bone marrow, bloodstream, lymph nodes, liver or spleen. Because the bone marrow is crowded with DLBCL cells too young to work properly, your normal blood cells will be affected. Supportive treatment may include things like you having blood or platelet transfusions on a ward or in an intravenous infusion suite in the hospital. You may have antibiotics to prevent or treat infections.
It may involve a consultation with a specialised care team or even palliative care. It can also be having conversations about future care, which is called Advanced Care Planning. These things are part of multidisciplinary management of lymphoma.
Supportive care can include palliative care which helps to improve your symptoms and side-effects, as well as end of life care if needed
It is important to know that the Palliative Care team can be called on at any time during your treatment pathway not just at the end of life. They can help control and manage symptoms (like hard to control pain and nausea) you might be experiencing as a result of your disease or its treatment.
If you and your doctor decide to use supportive care or stop curative treatment for your lymphoma, many things can be done to help you to stay as healthy and comfortable as possible for some time.
Radiation therapy is a cancer treatment that uses high doses of radiation to kill lymphoma cells and shrink tumours. Before having radiation, you will have a planning session. This session is important for the radiation therapists to plan how to target the radiation to the lymphoma, and avoid damaging healthy cells. Radiation therapy usually lasts between 2-4 weeks. During this time, you will need to go to the radiation centre everyday (Monday-Friday) for treatment.
*If you live a long way from the radiation centre and need help with a place to stay during treatment, please talk to your doctor or nurse about what help is available to you. You can also contact the Cancer Council or Leukemia Foundation in your state and see if they can help with somewhere to stay.
You might have these medications as a tablet and/ or be given as a drip (infusion) into your vein (into your bloodstream) at a cancer clinic or hospital. Several different chemo medications may be combined with an immunotherapy medicine. Chemo kills fast growing cells so can also affect some of your good cells that grow fast causing side effects.
You may have a MAB infusion at a cancer clinic or hospital. MABs attach to the lymphoma cell and attract other diseases fighting white blood cells and proteins to the cancer so your own immune system can fight the DLBCL.
MABS will only work if you have specific proteins or markers on your lymphoma cells. A common marker in DLBCL is CD20. If you have this marker you may benefit from treatment with a MAB.
Immune checkpoint inhibitors (ICIs) are a newer type of monoclonal antibody (MAB) and work a little differently to other MABS.
ICIs work when your tumour cells develop “immune checkpoints” on them which are usually only found on your healthy cells. The immuen checkpoint tells your immune system that the cell is healthy and normal, so your immune system leaves it alone.
ICIs work by blocking the immune checkpoint so your lymphoma cells can no longer pretend to be healthy, normal cells. This allows your own immune system to recognise them as cancerous, and begin an attack against them.
Chemotherapy combined with a MAB (for example, rituximab).
You may take these as a tablet or infusion into your vein. Oral therapies may be taken at home, though some will require a short hospital stay. If you have an infusion, you may have it at a day clinic or in a hospital. Targeted therapies attach to the lymphoma cell and block signals it needs to grow and produce more cells. This stops the cancer from growing and causes the lymphoma cells to die off.
A stem cell or bone marrow transplant is done to replace your diseased bone marrow with new stem cells that can grow into new healthy blood cells. Bone marrow transplants are usually only done for children with DLBCL, while stem cell transplants are done for both children adults.
In a bone marrow transplant, stem cells are removed straight from the bone marrow, where as with a stem cell transplant, the stem cells are removed from the blood.
The stem cells may be removed from a donor or collected from you after you’ve had chemotherapy.
If you the stem cells come from a donor, it is called an allogeneic stem cell transplant.
If your own stem cells are collected, it is called an autologous stem cell transplant.
Stem cells are collected through a procedure called apheresis. You (or your donor) will be connected up to an apheresis machine and your blood will be removed, the stem cells separated and collected into a bag, and then the rest of your blood is returned to you.
Before the procedure, you will get high-dose chemotherapy or full-body radiotherapy to kill off all your lymphoma cells. However this high dose treatment will also kill off all the cells in your bone marrow. So the collected stem cells will then be returned to you (transplanted). This happens in much the same was as blood transfusion is given, through a drip into your vein.

CAR T-cell therapy is a newer treatment that will only be offered if you have already had at least two other treatments for your DLBCL.
In some cases, you may be able to access CAR T-cell therapy by joining a clinical trial.
CAR T-cell therapy involves an initial procedure similar to a stem cell transplant, where your T-cell lymphocytes are removed from you blood during an apheresis procedure. Like you B-cell lymphocytes, T-cells are part of your immune system and work with your B-cells to protect you from disease and illness.
When the T-cells are removed, they are sent to a laboratory where they are re-engineered. This happens by joining the T-cell to an antigen that helps it recognise the lymphoma more clearly and fight it more effectively.
Chimeric means having parts with different origins so the joining of an antigen to the T-cell makes it chimeric.
Once the T-cells have been re-engineered they will be returned to you to start fighting the lymphoma.


